{kind=link}
The studies – TARGET FFR and DEFINE-FLOW – arrived sequentially in a groundbreaking session today at TCT Connect 2020.
TARGET FFR found that physiologically controlled PCI did not result in a greater proportion of patients with an optimal FFR ≥ 0.90 in treated vessels; However, the strategy reduced the proportion of patients with a remaining FFR ≤ 0.80. DEFINE-FLOW meanwhile brought the Coronary Flow Reserve (CFR) into the picture as a possible addition to FFR before PCI. Essentially, though complicated, the study found that even a high CFR flow did not negate the importance of a low FFR in determining which cases could be safely deferred.
“We need to pay more attention to the exact physiology we are measuring and what it means,” said Dr. DE LINE Gould (UT Health Science Center, Houston, TX) speaking to the press yesterday.
Indeed, physiological tests are not just a research tool. The results have clinical consequences. Damien Collison, MB BCh (National Golden Jubilee Hospital, Glasgow, Scotland) presented the TARGET FFR results in the “Main Arena” of TCT and said that below average PCI results could explain why up to 38% of patients 1 year after the Treatment still report angina.
He found that the registration data showed high variability in the final FFR, with 21% to 100% of patients achieving scores ≥ 0.90, which was associated with a lower risk of repeated PCI and MACE. “Maybe more worrying,” said Collison. Somewhere between 1% and 36% of patients have FFRs after PCI of 0.80 or less, he found.
SOUL FFR
Collison and colleagues admitted 260 patients to their center between March 2018 and 2019 and randomized them after angiographically successful PCI to receive an FFR-guided optimization or a blinded FFR assessment.
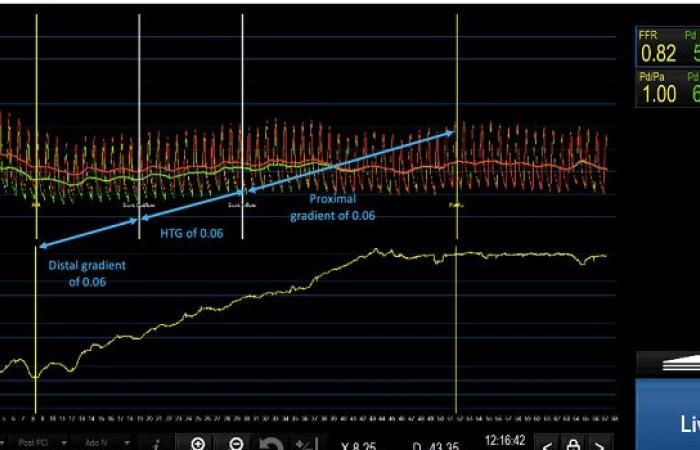
In the guided group, FFR retraction of stent vessels suggested targets for further optimization in 60 of the 131 patients (46%), with users performing additional post-dilation and / or stenting in 40 of these subjects (66%). These steps increased the mean FFR after PCI from 0.76 to 0.82, with a greater increase observed during the stent than after dilation, while the CFR increased from 3.0 to 4.0 (P. = 0,02).
“Not unexpectedly, additional PCI optimization measures were associated with a longer process duration in an analysis in the treated state [plus] higher doses of radiation, contrast, and adenosine, ”noted Collison, adding that there was“ no signal of undue harm ”related to complications.
Overall, the final FFR with FFR-driven optimization tended to be ≥ 0.90 (38.1% versus 28.1%; P. = 0.099). However, FFR values ≤ 0.80 were significantly less common in FFR-informed treatment after PCI (18.6% versus 29.8%; P. = 0.045). Consistent with previous registration data, the mean FFR values were lower when the target vessel was the LAD versus the left circumflex or right coronary arteries (0.80, 0.92 and 0.91, respectively). P.
The moderator of the session, Dr. Gregg W. Stone (Icahn School of Medicine at Mount Sinai, New York, NY) then asked why the operators decided not to perform further optimization in a third of patients whose FFR suggested improvement. In most cases, Collison replied, there were concerns about the safety of high pressure balloons after stenting, and in some cases the imaging guide may have indicated that no additional steps were required.
Allen Jeremias, MD (St. Francis Hospital, Roslyn, NY), lead author of the DEFINE-PCI In one study, he said he was “a bit shocked” to see that so few patients had optimal FFR after angiographic guidance alone. “It really shows the importance of controlling PCI before and after physiology,” he commented.
DEFINE THE RIVER
In recent years there has been a growing interest in better understanding microvascular abnormalities, Stone emphasized. “So it is a real pleasure to now look at one of the first real scientific studies to examine the importance of these topics,” he said, introducing DEFINE-FLOW.
The hypothesis of the study was that lesions with abnormal FFR ≤ 0.80 but intact CFR ≥ 2.0 would not achieve worse results with medical treatment, “compared to lesions with intact FFR and CFR”, Dr. Nils Johnson (UT Health Science Center). said in his presentation today.
DEFINE-FLOW researchers participated in 12 sites in six countries and examined 430 patients with 533 stable lesions who were simultaneously assessed with FFR and CFR. Only lesions with FFR ≤ 0.80 and CFR
After 2 years, the MACE rates (primary endpoint; death from all causes, MI and revascularization) differed in the four possible combinations, with the lowest rate in patients with FFR and CFR negative and the highest in patients with FFR and CFR positive . Target vessel failure (MI and revascularization) was again lowest in the patients with the best FFR and CFR values. It was highest in patients with low FFR but intact CFR.
Biennial results
| Medical therapy | PCI | |||
| FFR> 0,80 CFR ≥ 2.0 | FFR ≤ 0,80 CFR ≥ 2.0 | FFR> 0,80 CFR | FFR ≤ 0,80 CFR | |
| MORGENSTERN | 5,8% | 10,8% | 12,4% | 14,4% |
| TVF | 3,0% | 9,6% | 6,7% | 6,1% |
Lesions in vessels with abnormal FFR values ≤ 0.80 and normal CFR values ≥ 2.0 had a 2-year risk for MACE that was 5% higher than those who showed normal values for both FFR and CFR. This difference in MACE risk had no bearing on non-inferiority (P. = 0.065) – in other words, FFR mattered even in the face of normal CFR.
However, Johnson cautioned that there were limitations to consider – not just the observational study, particularly the comparison of treating lesions with a positive FFR, but also the negative CFR. This “really excludes our ability to make causal statements,” he said. Operators and patients were also not blind to the physiological results.
“DEFINE-FLOW is a hypothesis-generating study,” concluded Johnson, adding, “This study has at least taught me personally that we really need to distinguish between the flow to the downstream myocardium and the intracoronary pressure against the local plaque. I think it was natural to assume that the myocardium’s ability to increase its flow would really dominate symptoms and clinical events. DEFINE-FLOW suggests that local stress at the stenosis level further amplifies the natural history of atherosclerosis. “
We really need to distinguish between the flow to the downstream myocardium and the intracoronary pressure acting against the local plaque. Nils Johnson
Gould said at the press conference that “this little study is quite important for several, perhaps unclear, reasons”.
Its results undermine the idea that an adequate CFR could overcome an inadequate FFR, allowing for a PCI deferral. However, DEFINE-FLOW results are consistent with results from previous studies of quantitative perfusion in PET imaging, he explained. “The mechanistic explanation could be that the high stress flow (CFR) caused by mild to moderate stenosis or diffuse disease without a stenosis causes a drop in coronary pressure. The fluid dynamic equations relating coronary flow pressure predict heterogeneous arterial wall stresses associated with plaque instability, subendocardial ischemia, or both.
As a result, the high flow, low FFR lesion may indicate a less severe stenosis, but is still prone to plaque compared to low flow and low FFR lesions where the risk of plaque instability is even greater ” continued Gould.
A better understanding of the FFR / CFR thresholds associated with mortality and morbidity could influence study design and “possibly offset the ISCHEMIA and COURAGE studies [relied on] exact quantitative severity of the stricture, ”he said.
Roxana Mehran, MD (Icahn School of Medicine on Mount Sinai) moderated the press conference and said directly that she found the study “a little confusing”. Despite the lack of inferiority, Mehran drew attention in the statistical sense to cases with abnormal FFR ≤ 0.80 but intact CFR ≥ 2.0 as the main area for future studies and asked, “Do we have enough patients? [in DEFINE-FLOW] still to draw very important conclusions because of the permutations of the differential measurements? “
What emerges from large randomized studies – such as MOVE and Fame 2– Is treating low FFR lesions helpful, commented Dr. Chad Rammohan (Sutter Health, Mountainview, CA). It is investigating whether CFR can help determine which patients can safely postpone PCI despite the low FFR. “The process is a bit confusing for me as an interventional cardiologist,” he said, as did the “double negative” – that is, “not inferior” – in the conclusion.
The general message for now is that FFR should guide decision-making, Rammohan and Mehran agreed, as did Gould. “This study says that it is at this level that you have to trust the FFR [CFR]Said Gould. “I invented CFR. I would love to see how it works. But I’m a pretty cold blooded scientist. This attempt is very small [and] There are many restrictions. “He said a larger RCT is needed and that different CFR thresholds are being investigated.
For her part, Mehran called for additional studies on CFR, especially in diffuse diseases and in women. “There could also be some gender-specific microvasculature problems that could have an important impact on coronary flow reserve,” she noted.
These were the details of the FFR Insights Pre and Post PCI News: Fresh Thoughts for the Day. We hope that we managed to give you all the details and information. To keep up with all of our news, you can subscribe to the notification system or one of our various systems to receive everything that is new.
It’s also worth noting that the original news has been published and is available at de24.news. AlKhaleej Today’s editorial team has confirmed this and it has been changed and it may have been fully retransmitted or quoted and you can read it and follow this news from its main source.
These were the details of the news FFR Insights before and after PCI: Fresh food for thought for this day. We hope that we have succeeded by giving you the full details and information. To follow all our news, you can subscribe to the alerts system or to one of our different systems to provide you with all that is new.
It is also worth noting that the original news has been published and is available at de24.news and the editorial team at AlKhaleej Today has confirmed it and it has been modified, and it may have been completely transferred or quoted from it and you can read and follow this news from its main source.